
张建中主编推荐好文 — 跟骨内移截骨术避免神经损伤的安全区域: 尸体与影像学研究
来源:未知 | 发布时间:2016-04-15 15:02 | 浏览量:
跟骨内移截骨术避免神经损伤的安全区域:尸体与影像学研究
Safe Zone for Neural Structures in Medial Displacement Calcaneal Osteotomy: Aadaveric and Radiographic Investigation
Paul G. Talusan, MD1,2, Ezequiel Cata, MD1 ,Eric W. Tan, MD1,3,
Brent G. Parks, MSc1 , and Gregory P. Guyton,MD
Department of Orthopaedic Surgery, MedStar Union Memorial
Hospital, Baltimore, MD, USA
2 Department of Orthopaedic Surgery, University of
Michigan School of
Medicine, Ann Arbor, Michigan, USA
3Department of Orthopaedic Surgery, Keck School of Medicine,
University of Southern California, Los Angeles,California, USA
Abstract
Background: We aimed to define reference lines on standard lateral ankle radiographs that could be used intraoperatively to minimize iatrogenic nerve injury risk in medial displacement calcaneal osteotomy.
Methods: Forty cadaveric specimens were used. In 20 specimens, the sural, medial plantar (MP), and lateral plantar (LP) nerves were sutured to radiopaque wire, and a lateral ankle radiograph was obtained. On the radiograph, a line was drawn from the posterior superior apex of the calcaneal tuberosity to the origin of the plantar fascia and labeled as the “landmark line.” A parallel line was drawn 2 mm posterior to the most posterior nerve, and the area between these lines was defined as the safe zone. In 20 additional specimens, anosteotomy was performed 1 cm anterior to the landmark line using a percutaneous or open technique. Dissection was performed to assess for laceration of the sural, MP, LP, medial calcaneal (MC), or lateral calcaneal (LC) nerves.
Results: The safe zone was determined to be within the area 11.2 ± 2.7 mm anterior to the landmark line.After open osteotomy, lacerations were found in 3 of 10 MC nerves and 3 of 10 LC nerves. After percutaneous osteotomy, lacerations
were found in 2 of 10 MC nerves and 1 of 10 LC nerves. No lacerations of the sural, MP, or LP nerves were found with either osteotomy.
Conclusions: The safe zone extended 11.2 ± 2.7mm anterior to the described landmark line. The MC and LC nerves were always at risk during medial displacement calcaneal osteotomy.
Clinical Relevance: Nerve injury to both major and minor sensory nerves is likely underrecognized as a source of morbidity after calcaneal osteotomy. The current study provides a ready intraoperative guideline for minimizing this risk.
Foot & Ankle International 2015, Vol. 36(12) 1493–1498
跟骨内移截骨术据记载最早由 Gleich于1893 年完成, 在1971年后由 Koutsogiannis 推而广之, 用来治疗内翻扁平足畸形。
该术式通过将跟骨结节内移重建了足部负重力线, 同时也牵拉跟腱恢复相对正常的矢量力。在胫后肌功能不全的治疗中常与其他截骨术与肌腱转位术共同使用。跟骨内移截骨术重建后足力线也被用来在趾长屈肌腱转位术中保护趾长屈肌腱。
但是该术式也存在以下并发症的风险:延长伤口愈合,伤口感染以及切口区域感觉障碍。 其中感觉异常是广大医患特别注意的并发症, Wacker 报道 44 例行跟骨内移截骨术的患者中有 3 例出现了外侧感觉减退; Abbasian 发现 12%的患者在术后会出现皮肤感觉异常; 而 Kheir 报道在使用高速低扭矩磨钻的经皮跟骨内移截骨术中较少发生皮肤感觉异常。考虑到感觉异常的原因很大程度上来自周围神经的损伤,所以标定跟骨截骨的安全区域十分重要。 Myerson 指出应于距骨后突后方1cm 截骨, Greene 则推荐在腓骨滑车后方5mm内截骨, Bruce 认为前方跟骨截骨距胫神经4mm,后方截骨距胫神经14.2mm。尽管已有这些研究,但还不足以认定跟骨截骨的精确的最佳位置。
本研究选取了 40 只新鲜-冷冻的足标本,尸体平均年龄 78.1 岁, 其中 18 男, 22 女。 用可显影金属线绑定于腓肠神经、胫神经、足底内外侧神经上,然后行 X 线透视。 观察各条神经和骨的关系。 通过开放和经皮的跟骨截骨分别观察神经损伤以及神经和截骨平面的关系。


A 线是标志线,显示自跟骨结节后上方向跖筋膜起点处走形。
B 线是 A 线的平行线,距最靠后的神经后方 2mm, A线到 B 线之间的区域为安全区(图中阴影区)。
如患者曾行 Haglund 畸形骨赘清理术,跟骨后上结节已切除,很难用以上方法定位标志线,需按以下方法定位 A 线(标志线):

A 线是自 Gissane 角向跟骨结节最后方划的一条线,
B 线是平行于截骨方向的直线,它位于 A 线从 Gissane角向远端走行的 60%处。
安全区为 B 线近端 5.6mm 的区域内 (图中阴影区)。
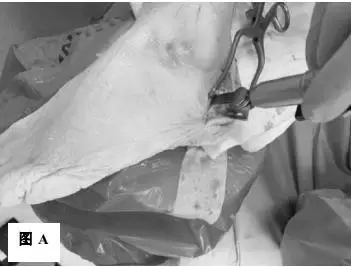

选定安全区后,在此区域内截骨。 传统的开放手术使用摆锯截骨(图 A),经皮截骨术则要使用高速低扭矩磨钻(图 B)。
结果:
本实验中,无论用什么截骨方法,都没有损伤腓肠神经、足底内外侧神经的主干。 表1示开放和经皮跟骨截骨神经损伤发生的数量。
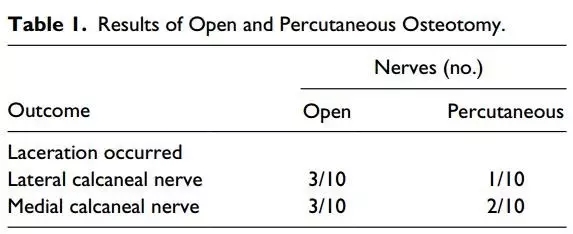
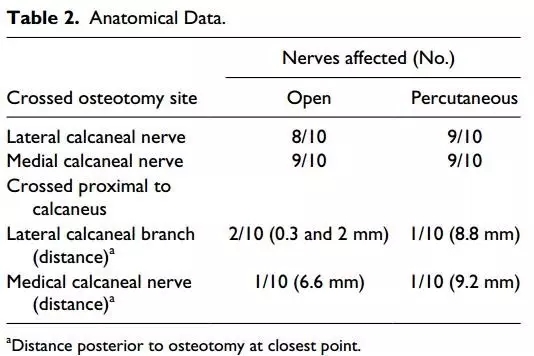
表2示 经过开放和经皮截骨术后,解剖尸体组织观察截骨平面和神经的距离。
结论:
1. 安全区域位于标志线近端(前方) 11.2 ± 2.7 mm
2. 该安全区为跟骨截骨避免损伤足底内外侧神经和腓肠神经提供的参考依据
3. 但无论截骨部位如何改变,都有损伤神经的可能。
专家点评:
在跟骨截骨术中,神经的损伤是一个常见的潜在并发症。本研究通过尸体研究,为我们提出了避免损伤神经的安全截骨的概念,对临床有所帮助。
我们目前的跟骨内移截骨术,多采用外侧切口。在显露时存在损伤腓肠神经的可能,应在切开时予以识别并牵开保护。 在截骨面的对侧,有可能损伤胫神经及其分支。 关于术中截骨的位置, Myerson 提倡的截骨区( 距骨后突后方 1cm) 有利于同时行腓骨肌腱移位,但太靠近足底内外侧神经,似损伤神经风险较大; 我们认为应避开足底内外侧神经一定距离,向远端直到跟骨结节处,这一区域作为截骨位置较为稳妥且易于操作。 但太靠近跟骨结节,可能会造成移位的困难。
需要注意的是: 截骨操作时, 使用摆锯时应注意截骨到对侧皮质时的突破感。 如无明显突破感, 如无突破感时,不要贸然深入,可以使用骨刀慢慢截断对侧皮质。
但由于本研究是尸体解剖研究,无法对腓肠神经损伤及其它神经损伤的临床结果进行评价。总之,虽然目前并无准确统计资料显示跟骨内移截骨术造成神经损伤的发生率,但应当有一个“安全区”的概念,这对减少截骨神经损伤的风险将大有裨益。
Safe Zone for Neural Structures in Medial Displacement Calcaneal Osteotomy: Aadaveric and Radiographic Investigation
Paul G. Talusan, MD1,2, Ezequiel Cata, MD1 ,Eric W. Tan, MD1,3,
Brent G. Parks, MSc1 , and Gregory P. Guyton,MD
Department of Orthopaedic Surgery, MedStar Union Memorial
Hospital, Baltimore, MD, USA
2 Department of Orthopaedic Surgery, University of
Michigan School of
Medicine, Ann Arbor, Michigan, USA
3Department of Orthopaedic Surgery, Keck School of Medicine,
University of Southern California, Los Angeles,California, USA
Abstract
Background: We aimed to define reference lines on standard lateral ankle radiographs that could be used intraoperatively to minimize iatrogenic nerve injury risk in medial displacement calcaneal osteotomy.
Methods: Forty cadaveric specimens were used. In 20 specimens, the sural, medial plantar (MP), and lateral plantar (LP) nerves were sutured to radiopaque wire, and a lateral ankle radiograph was obtained. On the radiograph, a line was drawn from the posterior superior apex of the calcaneal tuberosity to the origin of the plantar fascia and labeled as the “landmark line.” A parallel line was drawn 2 mm posterior to the most posterior nerve, and the area between these lines was defined as the safe zone. In 20 additional specimens, anosteotomy was performed 1 cm anterior to the landmark line using a percutaneous or open technique. Dissection was performed to assess for laceration of the sural, MP, LP, medial calcaneal (MC), or lateral calcaneal (LC) nerves.
Results: The safe zone was determined to be within the area 11.2 ± 2.7 mm anterior to the landmark line.After open osteotomy, lacerations were found in 3 of 10 MC nerves and 3 of 10 LC nerves. After percutaneous osteotomy, lacerations
were found in 2 of 10 MC nerves and 1 of 10 LC nerves. No lacerations of the sural, MP, or LP nerves were found with either osteotomy.
Conclusions: The safe zone extended 11.2 ± 2.7mm anterior to the described landmark line. The MC and LC nerves were always at risk during medial displacement calcaneal osteotomy.
Clinical Relevance: Nerve injury to both major and minor sensory nerves is likely underrecognized as a source of morbidity after calcaneal osteotomy. The current study provides a ready intraoperative guideline for minimizing this risk.
Foot & Ankle International 2015, Vol. 36(12) 1493–1498
跟骨内移截骨术据记载最早由 Gleich于1893 年完成, 在1971年后由 Koutsogiannis 推而广之, 用来治疗内翻扁平足畸形。
该术式通过将跟骨结节内移重建了足部负重力线, 同时也牵拉跟腱恢复相对正常的矢量力。在胫后肌功能不全的治疗中常与其他截骨术与肌腱转位术共同使用。跟骨内移截骨术重建后足力线也被用来在趾长屈肌腱转位术中保护趾长屈肌腱。
但是该术式也存在以下并发症的风险:延长伤口愈合,伤口感染以及切口区域感觉障碍。 其中感觉异常是广大医患特别注意的并发症, Wacker 报道 44 例行跟骨内移截骨术的患者中有 3 例出现了外侧感觉减退; Abbasian 发现 12%的患者在术后会出现皮肤感觉异常; 而 Kheir 报道在使用高速低扭矩磨钻的经皮跟骨内移截骨术中较少发生皮肤感觉异常。考虑到感觉异常的原因很大程度上来自周围神经的损伤,所以标定跟骨截骨的安全区域十分重要。 Myerson 指出应于距骨后突后方1cm 截骨, Greene 则推荐在腓骨滑车后方5mm内截骨, Bruce 认为前方跟骨截骨距胫神经4mm,后方截骨距胫神经14.2mm。尽管已有这些研究,但还不足以认定跟骨截骨的精确的最佳位置。
本研究选取了 40 只新鲜-冷冻的足标本,尸体平均年龄 78.1 岁, 其中 18 男, 22 女。 用可显影金属线绑定于腓肠神经、胫神经、足底内外侧神经上,然后行 X 线透视。 观察各条神经和骨的关系。 通过开放和经皮的跟骨截骨分别观察神经损伤以及神经和截骨平面的关系。
A 线是标志线,显示自跟骨结节后上方向跖筋膜起点处走形。
B 线是 A 线的平行线,距最靠后的神经后方 2mm, A线到 B 线之间的区域为安全区(图中阴影区)。
如患者曾行 Haglund 畸形骨赘清理术,跟骨后上结节已切除,很难用以上方法定位标志线,需按以下方法定位 A 线(标志线):
A 线是自 Gissane 角向跟骨结节最后方划的一条线,
B 线是平行于截骨方向的直线,它位于 A 线从 Gissane角向远端走行的 60%处。
安全区为 B 线近端 5.6mm 的区域内 (图中阴影区)。
选定安全区后,在此区域内截骨。 传统的开放手术使用摆锯截骨(图 A),经皮截骨术则要使用高速低扭矩磨钻(图 B)。
结果:
本实验中,无论用什么截骨方法,都没有损伤腓肠神经、足底内外侧神经的主干。 表1示开放和经皮跟骨截骨神经损伤发生的数量。
表2示 经过开放和经皮截骨术后,解剖尸体组织观察截骨平面和神经的距离。
结论:
1. 安全区域位于标志线近端(前方) 11.2 ± 2.7 mm
2. 该安全区为跟骨截骨避免损伤足底内外侧神经和腓肠神经提供的参考依据
3. 但无论截骨部位如何改变,都有损伤神经的可能。
专家点评:
在跟骨截骨术中,神经的损伤是一个常见的潜在并发症。本研究通过尸体研究,为我们提出了避免损伤神经的安全截骨的概念,对临床有所帮助。
我们目前的跟骨内移截骨术,多采用外侧切口。在显露时存在损伤腓肠神经的可能,应在切开时予以识别并牵开保护。 在截骨面的对侧,有可能损伤胫神经及其分支。 关于术中截骨的位置, Myerson 提倡的截骨区( 距骨后突后方 1cm) 有利于同时行腓骨肌腱移位,但太靠近足底内外侧神经,似损伤神经风险较大; 我们认为应避开足底内外侧神经一定距离,向远端直到跟骨结节处,这一区域作为截骨位置较为稳妥且易于操作。 但太靠近跟骨结节,可能会造成移位的困难。
需要注意的是: 截骨操作时, 使用摆锯时应注意截骨到对侧皮质时的突破感。 如无明显突破感, 如无突破感时,不要贸然深入,可以使用骨刀慢慢截断对侧皮质。
但由于本研究是尸体解剖研究,无法对腓肠神经损伤及其它神经损伤的临床结果进行评价。总之,虽然目前并无准确统计资料显示跟骨内移截骨术造成神经损伤的发生率,但应当有一个“安全区”的概念,这对减少截骨神经损伤的风险将大有裨益。
声明:本网站部分内容来源于网络,仅代表网络观点,如有侵权请及时与我方联系。




 扫一扫 关注玖玖骨科
扫一扫 关注玖玖骨科